|
The following article was sourced from a Wikipedia page at the following address: BOTULINUM TOXIN Botulinum toxin (BTX) is a neurotoxic protein produced by the bacterium Clostridium botulinum and related species. It is also produced commercially for medical, cosmetic, and research use. There are two main commercial types: botulinum toxin type A and botulinum toxin type B. Infection with the bacterium may result in a potentially fatal disease called botulism. Botulinum toxin type A and B is used in medicine for, among others, upper motor neuron syndrome, focal hyperhidrosis, blepharospasm, strabismus, chronic migraine and bruxism. It is also widely used in cosmetic treatments. The U.S. Food and Drug Administration requires the toxin to carry a boxed warning including a warning that locally administered toxin may spread from the injection site to other areas of the body, causing symptoms similar to those of botulism poisoning. The warning was the result of deaths associated with its uses. The commercial form is marketed under the brand-name, Botox among others. USES
Medical uses It is used in the treatment of spasms and dystonias. The conditions approved for treatment with botulinum toxin include:
Other adult uses of botulinum toxin type A include:
Uses of botulinum toxin type A in children include:
Emerging uses for botulinum toxin type A include chronic musculoskeletal pain.
Cosmetic ADVERSE EFFECTS
Off-target effects Adverse events or reactions from cosmetic use include facial paralysis resulting in inappropriate facial expression, drooping eyelid, and double vision, bruising, swelling, or redness at the site of injection, headaches, dysphagia, flu-like syndromes, blurred vision, dry mouth, fatigue, and allergic reactions. Cosmetic treatments are of limited duration; they can be as short as six weeks, but can last from 2–3 months; hence paralysis side-effects can have the same durations. The results of inappropriate facial expression, drooping eyelid, and double vision are foremost, but the list extends to uneven smiling, and loss of the ability to close ones eyes; at least in some cases, these effects are reported to dissipate in the weeks after treatment. Bruising at the site of injection is not a side effect of the toxin but rather of the mode of administration, and is reported as preventable if the clinician applies pressure to the injection site; when it occurs, it is reported in specific cases to last 7–11 days. When injecting the masseter muscle of the jaw, loss of muscle function can result in a loss or reduction of power to chew solid foods. Individuals who are pregnant, have egg allergies, or a neuromuscular disorder are advised to avoid botulinum toxin drugs, and breastfeeding mothers are advised to consult their doctors. The psychological and emotional consequences associated with cosmetic treatments is not yet well documented, and reports are not yet consistent. A study of treatment of glabellar lines with consequent reduction of ability to frown correlated with a "more positive mood[s]", while a study on the treatment of "crow's feet" or "laughter lines" suggested the opposite effect as a consequence of the impact of the treatment on the patient's ability to smile.
Poisoning The case fatality rate for botulinum poisoning between 1950 and 1996 was 15.5%, down from about 60% over the previous 50 years. Death is generally secondary to respiratory failure due to paralysis of the respiratory muscles, so treatment consists of antitoxin administration and artificial ventilation until the neurotoxins are excreted or metabolised. If initiated on time, these treatments are quite effective, although antisera can not affect toxin polypeptides that have already entered cells. Occasionally, functional recovery may take several weeks to months or more. Two primary botulinum antitoxins are available for treatment of botulism. Trivalent (A,B,E) botulinum antitoxin is derived from equine sources using whole antibodies (Fab and Fc portions). This antitoxin is available from the local health department via the CDC in the USA. The second antitoxin is Heptavalent (A,B,C,D,E,F,G) botulinum antitoxin, which is derived from "despeciated" equine IgG antibodies, which have had the Fc portion cleaved off, leaving the F(ab')2 portions. This less immunogenic antitoxin is effective against all known strains of botulism where not contraindicated, and is available from the United States Army. On June 1, 2006, the US Department of Health and Human Services awarded a $363 million contract with Cangene Corporation for 200,000 doses of heptavalent botulinum antitoxin over five years for delivery into the Strategic National Stockpile beginning in 2007.
Links to deaths In January 2008, a petition filed by Public Citizen with the FDA requested regulatory action concerning the possible spread of the effects of botulinum toxin injectable products, including Botox and Myobloc, from the site of injection to other parts of the body. On February 8, 2008, the FDA announced its conclusion that this class of drugs had "been linked in some cases to adverse reactions, including respiratory failure and death, following treatment of a variety of conditions using a wide range of doses," due to its ability to spread to areas distant from the site of the injection. The communication was a result of ongoing FDA safety reviews of the on-market product, and found adverse reactions associated with uses that were both FDA-approved and non-approved, the most severe being in children with cerebral palsy treated for limb spasticity (not approved for either adult or paediatric use). On April 30, 2009, based on a continuing safety evaluation of on-market botulinum toxin products, the FDA reported its conclusion that the prescribing information for Botox, Botox Cosmetic, and Myobloc must be updated to ensure their continued safe use. On July 31, 2009, FDA, under the authorities granted by the Food and Drug Administration Amendments Act of 2007, approved revisions to the prescribing information (see following). As well, on April 30, the FDA announced an update to its mandatory boxed warnings for four on-market products—Botox, Botox Cosmetic, Myobloc, and Dysport—and on July 31, it approved revisions to the prescribing information for the four drugs. In the revisions, it made clear that the effects of botulinum toxin may spread from the area of injection to other body areas, causing symptoms similar to those of botulism, including potentially life-threatening swallowing and breathing difficulties resulting in patient death. Most accumulated adverse reactions were again reported for paediatric palsy patients (off-label use, see above), though adverse reaction reports were also fielded for adult patients involved in both approved and unapproved uses; the FDA emphasized that at recommended/approved doses there were few serious adverse reactions for common, standard treatments for focal hyperhidrosis, blepharospasm, or strabismus, or for cosmetic/dermatologic treatments, e.g., for glabellar lines (i.e., when label instructions were followed). The FDA further emphasized that the activity units of each product do not interconvert, specifically that "different botulinum toxin products are not interchangeable, because the units used to measure the products are different," and required a change in the established drug names of older drugs, from:
doing so to "emphasize the differing dose to potency ratios of [each of] these products." A further FDA communication aimed at health care professionals reiterated the approved drugs for each adult indication:
These have been extended, through later announcement, to include:
which is defined for patients having a history of migraine, and experiencing a headache on most days of the month." In the 2009 communication to professionals, the FDA reiterated the foregoing adverse reaction observations and the possibility of "unexpected loss of strength or muscle weakness," leading to: double vision, blurred vision or drooping eyelids;
and that "swallowing and breathing difficulties can be life-threatening" (i.e., that there have been "deaths related to the effects of spread of botulinum toxin"). The communication to professionals reiterated that paediatric spasticity patients were at greatest risk from existing treatment practices, but also that approved and lower doses used to treat cervical dystonia and adult spasticity were also seen among the "cases of toxin spread," so that in all cases of drug administration, patients and their caregivers needed to: "Pay close attention for any signs or symptoms of adverse events. [and] Seek immediate medical attention… [in the case of] difficulty swallowing or talking, trouble breathing, or muscle weakness…" and that these events may occur "as late as several weeks after treatment."
Warning labels In April 2009, the FDA updated its mandatory boxed warning cautioning that the effects of the botulinum toxin may spread from the area of injection to other areas of the body, causing symptoms similar to those of botulism, and that these adverse reactions, which were more likely in cases ignoring approved use guidance and label directions, could result in patient death (see above).
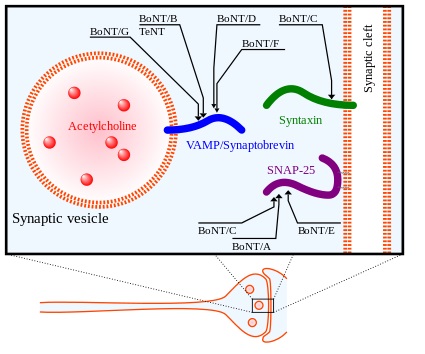
Target molecules of botulinum neurotoxin (abbreviated BoNT) and tetanus neurotoxin (TeNT), toxins acting inside the axon terminal, after Barr, Ashley, et al. The toxin produced by Clostridum species is a two-chain protein composed of a 100-kDa heavy chain polypeptide joined via disulfide bond to a 50-kDa light chain polypeptide. The eight serologically distinct toxin types "possess different tertiary structures and significant sequence divergence," and are designated A to G; six of the eight have subtypes, and five further subtypes of target molecules of botulinum A have been described. The A, B, and E serotypes cause human botulism, with the activities of types A and B enduring longest in vivo (from several weeks to months). The terminals of specific axons must internalize the toxin to cause paralysis, and the heavy chain of the toxins is implicated in targeting the toxin to such axon terminals; following the attachment of the toxin heavy chain to proteins on the surface of the terminals, toxin molecules enter the neurons by endocytosis. The light chain, which has zinc metalloprotease activity, is released from the endocytotic vesicles and reaches the cytoplasm. Specific serotypes of the toxin cleave synaptosomal-associated protein (25 kDa) (SNAP-25), a protein from the soluble N-ethylmaleimide-sensitive factor attachment receptor (SNARE) family involved in vesicle fusion and mediating release of neurotransmitter, in particular acetylcholine, from axon endings. Cleavage of the SNARE proteins inhibits release of acetylcholine. Hence, botulinum toxins A, B, and E specifically cleave SNAREs, preventing "neurosecretory vesicles" from docking/fusing with the interior surface of the plasma membrane of the nerve synapse, and so block release of neurotransmitter. In inhibiting acetylcholine release, nerve impulses are blocked, causing the flaccid (sagging) paralysis of muscles characteristic of botulism (versus the distinct spastic paralysis seen in tetanus). HISTORY Justinus Kerner described botulinum toxin as a "sausage poison" and "fatty poison" (from Latin botulus meaning "sausage"), because the bacterium that produces the toxin often caused poisoning by growing in improperly handled or prepared meat products. Kerner, a physician, first conceived a possible therapeutic use of botulinum toxin, and coined the name botulism. In 1897, Emile van Ermengem found the producer of the botulin toxin was a bacterium, which he named Clostridium botulinum. P.T. Snipe and Hermann Sommer purified the toxin for the first time In 1928. In 1949, Arnold Burgen's group experimentally discovered that botulinum toxin blocks neuromuscular transmission through decreased acetylcholine release. SOCIETY AND CULTURE
Economics
Bioterrorism The effects of botulinum toxin are distinguishable from those involving nerve agents insofar as botulism symptoms develop relatively slowly (over several days), while nerve agent effects are generally much more rapid, and can be instantaneous. Evidence suggests that nerve exposure (simulated by injection of atropine and pralidoxime) will increase mortality by enhancing botulin toxin's mechanism of toxicity. With regard to detection, current protocols using NBC detection equipment (such as M-8 paper or the ICAM) will not indicate a "positive" when samples containing botulinum toxin are tested. To confirm a diagnosis of botulinum toxin poisoning, therapeutically or to provide evidence in death investigations, botulinum toxin may be quantitated by immunoassay of human biological fluids; serum levels of 12–24 mouse LD50 units/mL have been detected in poisoned patients.
Manufacturers After the three primary U.S. manufacturers, there many reports of other sources of production. Xeomin, manufactured in Germany by Merz), is also available for both therapeutic and cosmetic use in the U.S. Lanzhou Institute of Biological Products in China is reported to manufacture a BTX-A product; BTX-A is also sold as Lantox and Prosigne on the global market. Neuronox, a BTX-A product, was introduced by Medy-Tox Inc. of South Korea in 2009; Neuronox is also markets as Siax in the U.S.
Toxin production Food-borne botulism results, indirectly, from ingestion of food contaminated with Clostridium spores, where exposure to an anaerobic environment allows the spores to germinate, after which the bacteria can multiply and produce toxin. Critically, it is ingestion of toxin rather than spores or vegetative bacteria that causes botulism. Botulism is nevertheless known to be transmitted through canned foods not cooked correctly before canning or after can opening, and so is preventable. Infant botulism cases arise chiefly as a result of environmental exposure and are therefore more difficult to prevent. Infant botulism arising from consumption of honey can be prevented by eliminating honey from diets of children less than 12 months old. Therapeutic and weaponisable forms of the toxin are sourced from strains of Clostridium where both the growth and toxin isolation are under specialized conditions.
Organism and toxin susceptibilities The botulinum toxin is denatured and thus deactivated at temperatures greater than 80 °C (176 °F). As a zinc metalloprotease (see below), the toxin's activity is also susceptible, post-exposure, to inhibition by protease inhibitors, e.g., zinc-coordinating hydroxamates. RESEARCH Alan Scott and Edward Schantz were the first to work on a standardized botulinum toxin preparation for therapeutic purposes, beginning in the late 1960s. Scott, working at Smith-Kettlewell Institute in 1963, used botulinum toxin type A (BTX-A) in monkey experiments. In 1980, Scott used BTX-A in a first human treatments of blepharospasm ("uncontrollable blinking") and strabismus, a condition in which the eyes are not properly aligned with each other ("crossed eyes"). In 1993, Scott, P.J. Pasricha, and colleagues showed botulinum toxin could be used for the treatment of achalasia, a spasm of the lower esophageal sphincter. In 1994, K.O. Bushara and D.M. Park were the first to demonstrate a non-muscular use of BTX-A in humans, with a demonstration that injections could inhibit conditions resulting in sweating.
Blepharospasm and strabismus In 1986, Scott's micromanufacturer and distributor of Botox was no longer able to supply the drug because of an inability to obtain product liability insurance. Patients became desperate, as supplies of Botox were gradually consumed, forcing him to abandon patients who would have been due for their next injection. For a period of four months, American blepharospasm patients had to arrange to have their injections performed by participating doctors at Canadian eye centers until the liability issues could be resolved. In December 1989, Botox, manufactured by Allergan, Inc., was approved by the US Food and Drug Administration (FDA) for the treatment of strabismus, blepharospasm, and hemifacial spasm in patients over 12 years old. Botox is not been approved for any paediatric use. It has, however, been used off-label by physicians for several conditions. including spastic conditions in paediatric patients with cerebral palsy, a therapeutic course that has resulted in patient deaths. In the case of treatment of infantile esotropia in patients younger than 12 years of age, several studies have yielded differing results.
Cosmetic
Upper motor neuron syndrome
Sweating
Cervical dystonia
Chronic migraine Since then, several randomized control trials have shown botulinum toxin type A to improve headache symptoms and quality of life when used prophylactically for patients with chronic migraine who exhibit headache characteristics consistent with: pressure perceived from outside source, shorter total duration of chronic migraines (<30 years), "detoxification" of patients with coexisting chronic daily headache due to medication overuse, and no current history of other preventive headache medications.
To read more about botox, please click on the following link: |
|
| Wikipedia: |
|